

CASE STUDY ANALYSIS: TANIA – EATING DISORDER
Introduction
Eating disorders are an increasing problem worldwide. In Australia, this healthcare-related issue is relevant for 9% of Australians and this number tends to grow, especially in terms of young females as this chronic disease is the third most common for this group of population (Slade 2012; Hay & Carriage 2012). Tania’s situation is the exact example of the above-indicated issue. Moreover, patients may experience either “inability to maintain normal body weight and a relentless pursuit of thinness” having anorexia nervosa (AN) (Bloss et al. 2011, p. 2222), so does Tania in a case study in question whose diagnosis is a restricted subtype of AN. Therefore, the paper is aimed to discuss AN eating disorder thoroughly providing an overview of this mental illness and the principles of recovery through the linkage of mental and physical health and in light of individual needs of the patient. In order to achieve this goal, the essay is based on three steps to be undertaken while analysing theoretical perspectives through the prism of the case discussed. First, the specific interventions and management within mental, physical and social dimensions for a given patient are to be considered. Second, modern factors regarding access to appropriate services, consumer and carer positions, and Indigenous mental health are further analysed. Third, communication strategies and other therapeutic modalities concerning maintenance of therapeutic patient-to-nurse relationship are discussed. As a result, the paper allows making relevant conclusions on the case study highlighted with potential application in similar instances accordingly.
A Comprehensive Understanding of Mental Health, Mental Illness and the Principles of Recovery
Mental health of each person determines the state of one’s overall well-being. In particular, a person can be called mentally healthy in case he or she is capable to evaluate own abilities in terms of being capable to encounter and deal with normal stresses on daily basis, work productively, and contribute to community enhancement in this way or another (Norman & Ryrie 2013, p. 3). On the contrary, occurrence of a mental illness in an individual involves inconsistencies within different dimensions of human existence with regard to subjective and objective correlations in self-to-community ratio depending on a type of illness as summarized in Figure 1 (Norman & Ryrie 2013, p. 4):
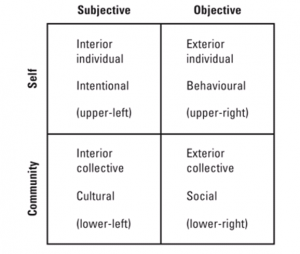
Figure 1: A framework of human experience
With relation to AN, all four constituents of the above-indicated framework can be clearly distinguished. In terms of intentional self level, Tania has such symptoms as “self-criticism” concerning her weight “associated with being a failure, flawed and inferior” (Gale, Gilbert, Read & Goss 2014, p. 2). In this regard, she has developed certain psychological signs of this disease, including feeling inadequate in meal times, obsession with a distorted body image with respect to her own one and her dissatisfaction with this issue, decreased self esteem, to list a few. As a result, the previously underlined characteristics led to behavioural changes. Namely, Tania constantly practices dieting for about 9 years, avoids meals with her family while preparing food for others obsessively, and does exercises excessively among others. Her behaviour is cognitively inflexible whereas it lasts for a sufficient period of time already (Tchanturie et al. 2012, p. 1). Conversely, its non-normality expands with time leading to deeper obsession with feeling fat while being actually underweight.
It is necessary to note that there is no evident genetic predisposition of the patient to this illness. However, inter-family relationships cannot be called smooth and too trustworthy due to parents being busy with their work all the time. Specifically, it is explicit from Tania’s relations with her brother who she finds to be “outgoing” and “popular” as it has been mentioned in the case study. Moreover, they study within one professional direction, which also emphasises “sibling rivalry” (Gale et al. 2014, p. 2) as one of the key determinants of her disorder. Since her obsessive experiencing of this state is long-lasting, her parents should have pay close attention to this fact as they are doctors, though the lack of communication in the family has resulted into Tania’s complete alienation.
Drawing upon these circumstances, the patient does not seek for treatment or at least help but rejects it. This is due to that the assistance has not being offered timely, at the initial stage of the disease. In this case, the entire family should be involved in the recovery process by means of family interventions focused explicitly on eating disorders (Norman & Ryrie 2013). Foremost, a nursing practitioner is to assess and detect the risks for Tania’s health. For instance, this is to be done by means of the computed Wisconsin Card Sorting Task (WCST) requiring one to sort stimulus cards in accordance with own beliefs on the issue (Tchanturia et al. 2012). Her long-lasting dieting obsession with related concerns may be already close to suicidal mood which is relevant to such disorders (Gales et al. 2014; Bloss et al. 2011). She has already encountered difficulties with regard to her physical health, such as gastritis and possible heart-related issues. Thus, this aspect is to be wisely used as a supportive argument in a well thought out strategy linked to a necessity to change Tania’s attitudes and behaviour. Also, persuasion should be linked to a range of other potential health issues that may arise in case AN will be left as it is.
What is more, a holistic approach is to be used in this case since mental health and well-being cannot be ensured by curing body solely. Therefore, the nurse has to establish a strategy on the grounds of the defined earlier constituents of person’s well-being, such as maintenance of strong emotional intelligence and productive work for self, family and community good. There is a number of successful recovery programs developed, though Tania’s case presupposes a specific one, with regard to her personal features and characteristics. For instance, cognitive behaviour therapy (CBT) is one of the most popular and proved to be effective to a great extent (Norman & Ryrie 2013). It involves gradual intervention in terms of thorough comprehension of AN as a health concern, recognition of own strengths to overcome this obstacle, establish specified beliefs and self-management strategies among other issues (see Appendix A). At the same time, the severity of Tania’s state and her long-lasting experiencing of this disorder makes it doubtful to achieve the success of this approach easily. Therefore, the CBT should be expanded and strengthened by a more up-to-date approach, such as compassion focused therapy (CFT) that is devoted to a more in-depth analysis of the case in question allowing to involve family members in the process as required by the circumstances discussed (Gales et al. 2014).

Therefore, a proposed intervention is to be grounded on the following elements:
- A family meeting (both parents at least) within an AN group in the framework of CFT strategy in order they all could understand the severity of Tania’s state, its predetermining factors, all possible consequences, and assess the harm that one has already experienced and may potentially face if the issue will not be addressed (refer to Appendix A).
- Further, the CBT model is to be applied as a way to convince both the patient and her families that the problem is huge and it has to be resolved by all means possible. This part of the session has to be family-focused to avoid any inconveniences or shameful situations for Tania and ensure her family support. This phase should involve a conscious transition or even a paradigm shift for a person from own inferiority towards individual problem-solving as summarised in Table 2 (Appendix B).
- The above-indicated process ought to be also linked to enhancement of emotional intelligence as “the ability to effectively process, use, understand, and manage emotional information” (McCaffrey, Edwards & Fannon 2011, p. 187). With assistance of healthcare practitioners and family members, Tania will learn to distinguish risk factors for her health by means of own emotions, nurture personal beliefs on a conscious rather than obsessive level. Nevertheless, this process requires time to be developed as a reflex appropriate for both internal and external influences. In any case, the phase of emotional intelligence involvement is a sophisticated means to develop personal mental health well-being for the patient in line with maintenance of self-management recovery on daily basis. In this regard, several important feelings will be enhanced within the patient’s consciousness, including:
- “self-acceptance”;
- “positive relations with others” (openness and trust in communication with family members in Tania’s case);
- an ability to think for herself and resist obsession;
- identification of a life purpose;
- “personal growth” (Norman & Ryrie 2013, p. 6).
Client says about us
The Nexus between Mental Health with Physical Health
There is “no health without mental health” (Norman & Ryrie 2013, p. 3). In terms of the case study, Tania has already experienced the problems related to gastroenterological and cardiologic spheres. Drawing upon the theoretical rationale for AN disorders, the negative impacts on the physical condition of the patient are about to expand if the issue will not be addressed at hand. To illustrate, these areas include problems with kidneys, anemia, weakened immune system, osteoporosis, intestinal concerns, problems with menstruation cycles, a substantial risk of infertility, to list a few (Hay & Carriage 2012; Mitchison, Hay, Slewa-Younan & Mond 2012; Zeidner, Matthews & Roberts 2012). Owing to that AN is a chronic disorder, all aforementioned physical health concerns may progress into chronic stage as well. Moreover, recognition of this fact can result into adverse depression in the patient, which will eventually deepen the consequences of AN for the patient’s organism, such as disabilities, and make the treatment outcomes hard to be achieved (McCaffrey, Edwards & Fannon 2011). Also, suicidal attempts and death as potential consequences of AN can be observed oftentimes.
It follows that there is an urgent need to arrange a multi-sided treatment strategy for the patient, including careful examination of a cardiologist as recommended by a general practitioner, with appropriate analyses (e.g. a general blood test regarding anemia) and electrocardiogram to be made. This aspect is to be a starting point in Tania’s treatment. Whereas the young girl whose situation is discussed has more than free access to care since her parents are doctors themselves, the greatest barrier to receiving care is her unwillingness to apply for it. When persuading Tania that she needs appropriate care to mitigate the further harm for her health condition, it is relevant to refer to “recovery-orientated mental health system focus on commonality” as it has been proposed by Slade (2012) with relation to the triple nature of the problem.
First, the fact that the problem is of sociological character is to be underlined: namely, all individuals are alike and all can face similar health concerns. In contrast, Indigenous people can be referred to. Indeed, the statistics reveals that this Australian population group is vulnerable to eating disorders, though the accessibility to care in this regard is limited, especially in terms of remote areas of their habitat (Hay & Carriage 2012; Wilson & Zandberg 2012). By the same token, the majority of persons with AN, both Indigenous and non-Indigenous Australians, typically disregard seeking for treatment for at least eight years (Hay & Carriage 2012), the way Tania does.
Second, with the above reasoning, Tania should be convinced that she has an opportunity to obtain a mental-to-physical health and life balance. Hence, she has no right to ignore it in order to be empowered to further assist a wider community either in her professional sphere or with regard to the same health concerns by her life example guidance. In this way, it will be possible to emphasise psychological understanding of the issue under consideration: i.e. the aspect that she may become a more productive community member and make a difference in terms of addressing AN given her own situation. In this regard, she will be positioned not only as a consumer of healthcare services but also as the one who is capable to achieve her personal holistic mental well-being and enable others to follow this recovery path (Zeidner, Matthews & Roberts 2012).
Finally, attaining the aforementioned level of an all-embracing state of mental well-being is to underline “persistence of identity over time and space” as a constituent of the proposed approach in ensuring mental-to-physical health nexus (Slade 2012, p. 702). Therefore, the carer and consumers’ perspectives are intertwined in this regard because they enhance and empower one another when ascertaining the patient that “development and consolidation of one’s identity are central to recovery” (Slade 2012, p. 702).
Recognizing and Responding to the Mental Health Needs of the Identified Person
Undoubtedly, all previously argued options to address AN in Tania will be in vain if a well thought out, planned and administered treatment will not be maintained on the grounds of proper communication models. It is necessary to accent on that the recovery framework should not be a manifestation of indulgence to the patient or any controlling over her behavior since she has already opposed all previous attempts of her parents in so doing. Conversely, the emphasis in communication strategies as a way to establish trustworthy relationships between care-givers, the patient and her family members is to be put on well-reasoned and practically evidenced issues, though all information is to be revealed in a careful manner. For instance, it ought to be advisable to arrange the initial communication with the patient who is too “self-critique” and “shame-prone” (Gales et al. 2014, p. 2) after the physical examination Tania’s parents should be present during the process, but do not interfere with advises or remarks like “Didn’t I told you?” or “We were right that you are ill” etc. On the contrary, they have to position themselves as attentive listeners in this case, who are willing and sincerely support their daughter that she could balance her self-identity the way she would like to. The above conclusion has to be reached due to communication with a healthcare provider prior to a mutual conversation with Tania in order to mitigate the risk of a repetitive potential care denial from Tania and further worsening of the situation.
On the basis of the rationale provided, Tania’s recovery has to be self-defined (Norman & Ryrie 2013) and thoroughly grounded on her own strengths and capabilities in accordance with her mental needs and concerns. Indeed, a healthcare professional will communicate to the patient common issues and symptomatic related to AN as she is “resistant to treatment and lacks insight regarding the medical consequences of the disorder” (Boss et al. 2011, p. 222). In this way, she has to be the one who diagnoses herself by detecting similar symptoms in her own attitudes, beliefs and behaviour. The most important is that she has to be knowledgeable in severity of her disorder but showed positive outcomes and life-saving advantages of a properly administered care simultaneously (Norman & Ryrie 2013). The crucial thing is to convince her that she has came to healthcare facility in time, will receive timely care and constant family support in order to become self-managed and emotionally strong person that will be enabled to resist external forces with respect to AN and position herself as a emotionally intelligent individual (Slade 2012; Norman & Ryrie 2013). It is vital to ensure Tania that she is not alone, hopeless, and inadequate, but on the contrary, loved by all her family members and cared by professionals. Therefore, a specific family-focused eating disorder intervention has been recommended for implementation with regard to the case study. While family support will be granted, she will be convinced that her own strengths and self-education is the way to overcome this life-threatening issue by means of combined CBT and CFT sessions guided by professionals with appropriate skills and knowledge hand-in-hand with people facing similar difficulties in life.
Implications for Future Practice
Drawing upon the analysis, it is clear that AN is a serious medical concern that is to be addressed holistically in all aspect possible. In particular, there should be no distinguishing between formulating the recovery strategy based on either mental or physical health or well-being alone. Conversely, this disease requires in-depth knowledge and skills of a nurse in both fields, as well as thorough awareness in all-dimensional health consequences of the disorder. Also, there is a reasonable ratio to agree with the scholars, such as Slade (2012) and that the task Norman and Ryrie (2013) among others, that the nurse is to assist the patient in empowering one’s own personality in terms of dealing with the disease. Undoubtedly, treatment of mental disorder does not have to be positioned as further alienation and deepening inferiority of the patient on the grounds of her inadequacy in the world of normal people. In contrast, the patient has to be convinced that the one is strong enough to address it, the care is timely and both family and care-givers’ support is ensured, but one is to consciously realise a necessity for care and ongoing treatment. Whereas there are common symptoms of AN, such as anxiety, excessive self-criticism on the grounds of feeling fat when being underweight and shame-prone, individual needs and considerations should not be ignored but become a centrepiece for recovery strategy.
Conclusion
Summing up the discussion, it is to be noted that Tania faced a substantial mental disorder that is to be holistically addressed in order to achieve recovery. It is evident that mental well-being of the person, which is of multiple dimensions, is impossible without careful considering interrelation of mental and physical health of the individual. To illustrate, Tania is physically weak due to being underweight and mentally disabled because of aiming for thinness more and more. Therefore, she has to be convinced that administering care in her case is vital in order to mitigate health risks she has already encountered and eliminate further complications within both mental and physical health domains. Regardless of a range of approaches to AN care available, the treatment strategy is to be individual-need-based for every patient but holistically directed at nurturing self-management and emotional intelligence as favourable coping strategies.
You can Buy Case Study on this or any other topic at 123HelpMe.org. Don’t waste your time, order now!
Appendices
Appendix A
Table 1: A Sample CBT Framework for Addressing AN (Gale et al. 2014, p. 2)

Appendix B
Table 2: Composition of the recovery programme (Gale et al. 2014, p. 3)


